‘Does gum disease kill you?’ is a tough question. But it is pertinent. Because gum disease often does not appear as a direct cause of death, the real danger is that it shares the same ground with risks that grow silently in the rest of the body. We also know that severe infections that spread through the mouth can progress to fatal complications such as sepsis and airway obstruction. This is why it is not just gum.
Bleeding gums are not a simple bleeding
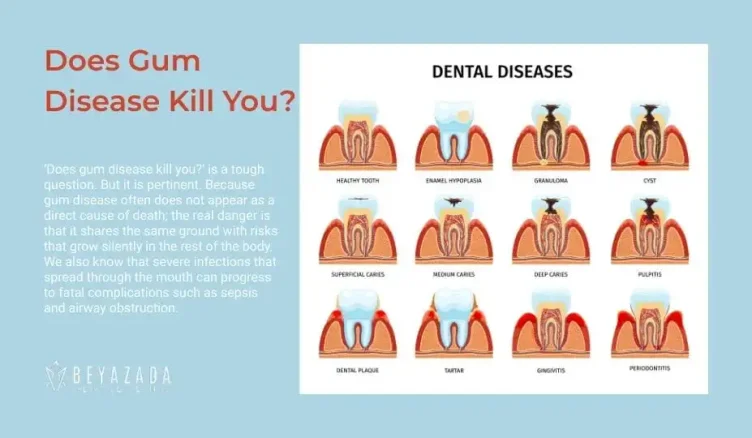
Healthy gums do not bleed. Bleeding is often the first sign of gingivitis, the inflammation that develops against bacterial plaque accumulated in the gum groove. Gingivitis can be reversible with proper care and professional support. However, if it is not managed in susceptible people, it can progress to periodontitis; at this stage, destruction of tooth-bearing tissues and bone begins.
Periodontitis does not only mean ‘tooth with the flesh removed’. The connective tissue and bone support around the tooth weaken; teeth may become loose, and tooth loss may occur. This affects both chewing function and quality of life. Moreover, periodontitis is common in society; studies have shown that its severe form is a common burden worldwide.
At this point, one fact should be clear: Oral health is part of general health. The World Health Organisation emphasises that oral diseases can lead to lifelong pain, loss of function and, in some cases, serious infections.
Mouth to blood: the mechanism of spread of inflammation
The key problem of periodontitis is the following: Deepened areas called ‘pockets’ form at the gingival margin. The inner surface of these pockets is inflamed and often ulcerated. In other words, it actually acts like an open entrance door. In severe, untreated periodontitis, it has even been reported that this ulcerated surface area can reach a significant size.
Two things ‘touch’ the systemic circulation from this area:
Firstly, the passage of bacteria and bacterial products (e.g. LPS) into the bloodstream. Transient bacteraemia can occur even in ordinary moments of everyday life (such as brushing teeth); this is especially likely as plaque build-up and gingivitis increase.
Secondly, inflammatory mediators produced by the immune system enter the bloodstream. Periodontitis can increase the burden of ‘low-level systemic inflammation’; the increase in markers such as CRP and its decrease after periodontal treatment have been repeatedly shown in many reviews.
Historically, this idea has its roots in the ‘focal infection theory’: The idea that foci of chronic infection in the mouth could affect distant organs. Today we are more cautious. Not every correlation is causation. But the biological possibility is not empty. What we talk about in periodontal medicine is the triad of bacterial transmission + chronic inflammation + common risk factors.
At this point, we put the phrase ‘correlation ≠ causation’ on the table with a physician’s reflex. Chronic conditions such as periodontitis and heart disease may occur more frequently in the same person because common determinants such as smoking, diet, socioeconomic conditions and access to health care feed both conditions. This is why even good studies struggle to prove causality.
Gum disease and heart health: The cardiovascular connection
One of the most fundamental processes in cardiovascular disease is atherosclerosis and the underlying inflammatory vascular response. The reason for discussing periodontitis here is twofold: the epidemiological relationship and the biological mechanism.
In its scientific statement of 2012, the American Heart Association clearly states that there are observational data supporting an independent association between periodontitis and atherosclerotic vascular disease, but that causality has not been proven. In the same statement, it is emphasised that the two diseases share common risk factors such as smoking, age and diabetes.
This area remains topical. The Society’s update of 16 December 2025 highlights the expansion of the ‘association’ literature with new data, possible mechanisms (bacteraemia, possibility of vascular infection, systemic inflammation) and knowledge gaps.
So what is on the mechanism side? It has been reported that periodontitis can increase systemic inflammatory markers and that periodontal treatment can reduce this burden, with some studies reporting improvement in endothelial function over time. This forms a plausible biological bridge to ‘vascular health’. But it is too early to jump to the conclusion that ‘gum treatment prevents heart attacks’.
Diabetes, alzheimer’s disease and pregnancy: different rooms of the same fire
In this topic, I am addressing all three areas together because the basic common denominator is the same: chronic inflammatory burden, changes in the immune response and common risk factors.
Diabetes
There is a ‘two-way’ relationship between diabetes and periodontitis: Hyperglycaemia makes periodontal tissues more fragile. On the other hand, severe periodontitis can increase systemic inflammation, making glycaemic control more difficult.
The collaborative report published in the Journal of Periodontology summarises that severe periodontitis can adversely affect glycaemic control in diabetes, that the association with diabetes complications is strengthened as severity increases, and that mechanical periodontal treatment may be associated with a clinically significant reduction in HbA1c around 3 months.
There are also reviews of randomised trials that support this finding. Although measurement methods and patient profiles vary, some meta-analyses have reported a decrease in HbA1c after SRP (scaling and root planing). Let’s be honest here: Effect size varies from study to study, and long-term sustainability is not always clear. Nevertheless, the fact remains that periodontitis is an area ‘not to be ignored’ in diabetes management.
Alzheimer’s disease
Most studies reporting an association between periodontitis and Alzheimer’s disease are observational in nature. Systematic reviews and meta-analyses have reported higher odds ratios for Alzheimer’s disease in the presence of periodontitis. However, the same studies specifically note methodological limitations and uncertainty of causality. Although this field has strong hypotheses for a ‘possible biological link’, it requires more evidence for clinical certainty.
Pregnancy complications
We know that adverse pregnancy outcomes, such as low birth weight, preterm labour, and pre-eclampsia, are multifactorial. Periodontitis may add to this picture as a factor that may influence the inflammatory response in the foetal-maternal unit.
The joint EFP/AAP report discusses the epidemiological relationship and possible mechanisms. The important nuance is the same here: The same effect is not expected in every woman; the presence of periodontitis does not necessarily mean ‘it will be a problem’. But it should be taken into account in risk management.
Side note: There are also meta-analyses of the association of periodontitis with respiratory diseases; in particular, studies reporting associations with pneumonia, COPD and asthma have been published. This association is mostly observational, and intraoral biofilm management is of practical importance, especially in elderly individuals at high risk of swallowing aspiration.
Periodontal disease symptoms: Which signs should you take seriously?
The worst feature of periodontitis is that it has ‘few symptoms’ until it is very advanced. It is therefore dangerous to relax because there is no pain.
The most common periodontal disease symptoms we see in the Beyazada Dental Clinic in Antalya are the following:
- Bleeding gums (especially with brushin/flossing).
- Gingival redness, swelling, and tenderness when touched.
- Bad breath (permanent, including the odour described as ‘perio breath’).
- Gum recession, exposure of the root surface, hot-cold sensitivity.
- Teeth wobbling, gaps opening, change in bite.
- Pain/discomfort during chewing; ‘I can’t bite anything hard’ in some patients.
There are also symptoms with an emergency threshold: rapidly increasing swelling of the face/jaw, fever, weakness, marked limitation in opening the mouth, difficulty swallowing or difficulty breathing. These may be more than a simple dental problem. Oral infections can progress to complications such as sepsis and airway obstruction. Urgent assessment is required without waiting.
Preventing tooth loss: Early detection, professional cleaning and a sustainable routine
Let’s get the sentence right first: Periodontitis is not fate. But it is also not a condition that can be ‘cured at home with mouthwash’. The goal of treatment is to control inflammation, manage pocket depths and keep teeth in the mouth for the long term.
Guidelines recommend a stepwise approach to the treatment of periodontitis: behavioural modification and risk factor control, supragingival/subgingival cleaning (SRP, which most patients in the clinic call ‘deep cleaning’), surgical approaches when necessary, and supportive periodontal care as the most critical part. This care is to preserve the gains of treatment.
The practical reality for ‘preventing tooth loss’ is this: If care is interrupted after treatment, the disease returns. Long-term follow-up data have shown that deep pockets remaining after treatment can significantly increase the risk of tooth loss.
Here are some simple but indispensable home methods for gum disease:
Brushing twice a day with fluoride paste.
Daily interdental cleaning (flossing or a suitable interdental brush). Because the brush doesn’t get everywhere, and that’s often where the disease likes to go.
Quitting tobacco products. It significantly affects the risk of periodontitis and response to treatment.
If you have diabetes, take glycaemic control seriously; there is a bidirectional relationship with periodontitis.
On the professional side, the main issue is timing: If the disease is caught early, it is easier to reduce the risk of both bone loss and tooth loss. The periodontal care interval varies according to the individual; a risk-based plan is made (3-6 months is common in most clinics). The evidence for a ‘one right interval’ is not strong, but there is clinical rationale and observational data that regular care favours tooth retention.
And local reality: It is difficult to proceed without an examination. No matter how well you look below the gum line at home, you cannot fully assess it. So don’t stop at ‘just fine’. Get examined by a specialist periodontologist (local periodontist) nearby.